Nexium: Children 1 - 11 years: Gastroesophageal Reflux Disease (GERD): Treatment of erosive reflux esophagitis: Weight <20 kg: 10 mg once daily for 8 weeks.
Weight ≥20 kg: 10 mg or 20 mg once daily for 8 weeks.
Long-term management of patients with healed esophagitis to prevent relapse: 10 mg once daily.
Symptomatic treatment of gastroesophageal reflux disease (GERD): 10 mg once daily for up to 8 weeks.
Doses over 1 mg/kg/day have not been studied.
Children 0 - 1 year: Gastroesophageal Reflux Disease (GERD): Treatment of gastroesophageal reflux disease (GERD) diagnostically confirmed through pH probe or endoscopy.
1 - 11 months: Weight 3 kg to 5 kg: 2.5 mg once daily for up to 6 weeks.
Weight > 5 kg to 7.5 kg: 5 mg once daily for up to 6 weeks.
Weight >7.5 kg to 12 kg: 10 mg once daily for up to 6 weeks.
Doses over 1.33 mg/kg/day have not been studied.
0 - 1 month: Weight > 2.5 kg: 2.5 mg once daily for up to 4 weeks.
Impaired renal function: Dose adjustment is not required in patients with impaired renal function. Due to limited experience in patients with severe renal insufficiency, such patients should be treated with caution. (See Pharmacology: Pharmacokinetics under Actions.)
Impaired hepatic function: Dose adjustment is not required in patients with mild to moderate liver impairment. For patients with severe liver impairment, a maximum daily dose of 20 mg Esomeprazole (NEXIUM) should not be exceeded. (See Pharmacology: Pharmacokinetics under Actions.)
Tablet: The tablets should be swallowed whole with liquid.
They should not be chewed or crushed. The tablets can also be also dispersed in half a glass of non-carbonated water. No other liquids should be used. Stir until the tablets disintegrate and drink the liquid with the pellets immediately or within 30 minutes. Rinse the glass with half a glass of water and drink. The pellets must not be chewed or crushed.
For patients who cannot swallow, the tablet contents can be dispersed in non-carbonated water and administered through a gastric tube.
Adults: Gastroesophageal Reflux Disease (GERD): Treatment of erosive reflux esophagitis: 40 mg once daily for 4 weeks.
An additional 4 weeks treatment is recommended for patients in whom esophagitis has not healed or who have persistent symptoms.
Long-term management of patients with healed esophagitis to prevent relapse: 20 mg once daily.
Symptomatic treatment of GERD: 20 mg once daily in patients without esophagitis. If symptom control has not been achieved after 4 weeks, the patient should be further investigated. Once symptoms have resolved, subsequent symptom control can be achieved using an on demand regimen taking 20 mg once daily, when needed. In NSAID treated risk patients subsequent symptom control using on demand treatment is not recommended.
Patients requiring continued non-steroidal anti-inflammatory (NSAID) therapy: Treatment of upper gastrointestinal symptoms associated with NSAID therapy: 20 mg once daily in patients requiring NSAID therapy. If symptom control has not been achieved after 4 weeks, the patient should be further investigated.
Healing of gastric ulcers associated with NSAID therapy: 20 mg or 40 mg once daily for 4 to 8 weeks.
Prevention of gastric and duodenal ulcers associated with NSAID therapy in patients at risk: 20 mg or 40 mg once daily.
Patients requiring continued low dose aspirin therapy: Prevention of gastric and/or duodenal ulcers associated with low dose aspirin therapy in patients at risk: 20 mg or 40 mg once daily.
Maintenance of hemostasis and prevention of rebleeding of gastric or duodenal ulcers following treatment with Esomeprazole (NEXIUM) IV: 40 mg once daily for 4 weeks. The oral treatment period should be preceded by acid-suppression therapy with Esomeprazole (NEXIUM) IV 80 mg administered as bolus infusion over 30 minutes followed by a continuous intravenous infusion of 8 mg/hr given over 3 days (Refer to the Esomeprazole (NEXIUM) IV prescribing information as follows).
In combination with an appropriate antibacterial therapeutic regimen for the eradication of Helicobacter pylori and: healing of
Helicobacter pylori associated duodenal ulcer and prevention of relapse of peptic ulcers in patients with
Helicobacter pylori associated ulcers: 20 mg Esomeprazole (NEXIUM) with 1 g amoxicillin and 500 mg clarithromycin, all twice daily for 7 days.
Pathological hypersecretory conditions including Zollinger-Ellison syndrome and idiopathic hypersecretion: The recommended initial dosage is Esomeprazole (NEXIUM) 40 mg twice daily. The dosage should then be individually adjusted and treatment continued as long as clinically indicated. Doses up to 120 mg twice daily have been administered.
Children 12 - 18 years: Gastroesophageal Reflux Disease (GERD): Treatment of erosive reflux esophagitis: 40 mg once daily for 4 weeks.
An additional 4 weeks treatment is recommended for patients in whom esophagitis has not healed or who have persistent symptoms.
Long-term management of patients with healed esophagitis to prevent relapse: 20 mg once daily.
Symptomatic treatment of gastroesophageal reflux disease (GERD): 20 mg once daily in patients without esophagitis. If symptom control has not been achieved after 4 weeks, the patient should be further investigated. Once symptoms have resolved, subsequent symptom control can be achieved using 20 mg once daily under medical supervision.
Treatment of duodenal ulcer caused by H. Pylori: When selecting appropriate combination therapy, consideration should be given to official national, regional and local guidance regarding bacterial resistance, duration of treatment (most commonly 7 days but sometimes up to 14 days), and appropriate use of antibacterial agents.
The treatment should be supervised by a specialist.
The dosage recommendation for esomeprazole is the following: 20 mg twice daily for one week.
Elderly: Dose adjustment is not required in the elderly.
Granules: The contents of a 10 mg sachet should be emptied into a container containing a tablespoon (15 mL) of non-carbonated water. Stir the contents and leave for a few minutes to thicken. Stir again and drink within 30 minutes. If any material remains after drinking, add more water, stir, and drink immediately. In cases where there is a need to use two sachets, they may be mixed in a similar way adding twice the required amount of water.
For patients who have a nasogastric or gastric tube in place, the contents of a 10 mg sachet can be added to a syringe containing 15 mL of water. Immediately shake the syringe and leave for a few minutes to thicken. Shake the syringe and inject through the nasogastric or gastric tube, French size 6 or larger, within 30 minutes. Refill the syringe with an equal amount of water (15 mL) and shake and flush any remaining contents from the nasogastric or gastric tube into the stomach.
Alternatively, the suspension can be prepared first and then drawn up into a syringe. Empty the contents of the 10 mg sachet into 15 mL of water. Stir and leave for a few minutes to thicken. Stir again and then draw the suspension into a syringe. Inject through the enteric tube, French size 6 or larger, into the stomach within 30 minutes after reconstitution. Refill the syringe with an equal amount of water (15 mL). Shake and flush any remaining contents from the enteric tube into the stomach.
Adults and adolescent from the age of 12 years: For dosage in patients from the age of 12 years, reference is made to the Esomeprazole (NEXIUM) Tablet Prescribing Information.
Nexium IV: Gastroesophageal Reflux Disease (GERD): Adults: Treatment with Esomeprazole (NEXIUM) I.V. can be given for up to 10 days as part of a full treatment period for the specified indications. When oral therapy is possible or appropriate, intravenous therapy with Esomeprazole (NEXIUM) I.V. should be discontinued and the therapy should be continued orally.
Treatment of erosive reflux esophagitis: 40 mg once daily.
Long-term management of patients with healed esophagitis to prevent relapse: 20 mg once daily.
Symptomatic treatment of gastroesophageal reflux disease: 20 mg once daily in patients without esophagitis.
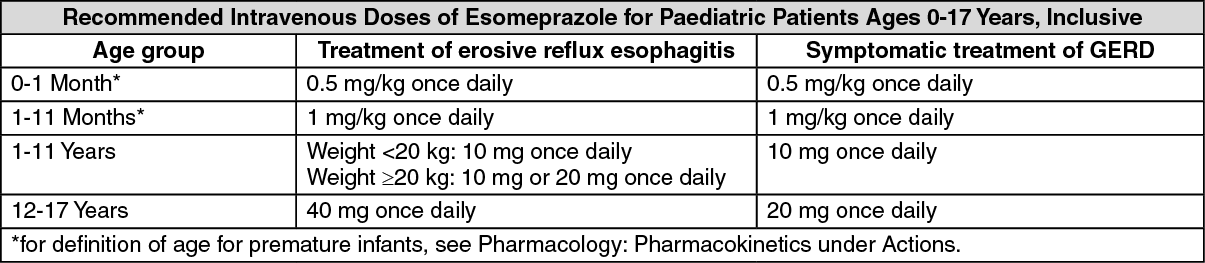
Children: Treatment with Esomeprazole (NEXIUM) I.V. can be given as part of a full treatment period for GERD. When oral therapy is possible or appropriate, intravenous therapy with Esomeprazole (NEXIUM) I.V. should be discontinued, and the therapy should be continued orally. Dosing recommendations are provided in the table as follows. (See table.)
 Click on icon to see table/diagram/image
Patients requiring continued non-steroidal anti-inflammatory (NSAID) therapy: Healing of gastric ulcers associated with NSAID therapy:
Click on icon to see table/diagram/image
Patients requiring continued non-steroidal anti-inflammatory (NSAID) therapy: Healing of gastric ulcers associated with NSAID therapy: 20 mg once daily.
Prevention of gastric and duodenal ulcers associated with non-steroidal anti-inflammatory (NSAID) therapy in patients at risk: 20 mg once daily.
Maintenance of hemostasis and prevention of rebleeding of gastric or duodenal ulcers: 80 mg administered as bolus infusion over 30 minutes followed by a continuous intravenous infusion of 8 mg/hr given over 3 days.
The parenteral treatment period should be followed by acid-suppression therapy with Esomeprazole (NEXIUM) 40 mg orally once daily for 4 weeks (Refer to the Esomeprazole (NEXIUM) Tablet prescribing information - Dosage & Administration previously).
Method of administration: Injection (40 mg vial): A solution for injection (8mg/mL) is prepared by adding 5 mL of 0.9% sodium chloride for intravenous use to the vial.
40 mg dose: 5 mL of the reconstituted solution (8mg/mL) should be given as an intravenous injection over a period of at least 3 minutes.
20 mg dose: 2.5 mL or half of the reconstituted solution (8mg/mL) should be given as an intravenous injection over a period of approximately 3 minutes.
10 mg dose (Children 1-11 years): 1.25 mL of the reconstituted solution (8 mg/mL) should be given as an intravenous injection over a period of at least 3 minutes.
1 mg/kg (Children 1-11 months*): A solution for injection (2 mg/mL) is prepared by adding 20 mL of 0.9% sodium chloride for intravenous use to the vial.
Calculate the volume of the reconstituted solution (2 mg/mL) for the required dose (1 mg/kg) and administer an intravenous injection over a period of at least 3 minutes.
0.5 mg/kg (Children 0-1 month*): A solution for injection (0.8 mg/mL) is prepared by adding 50 mL of 0.9% sodium chloride for intravenous use to the vial.
Calculate the volume of the reconstituted solution (0.8 mg/mL) for the required dose (0.5 mg/kg) and administer an intravenous injection over a period of at least 3 minutes.
*for definition of age for premature infants, see Pharmacology: Pharmacokinetics under Actions.
Infusion (40 mg vial): A solution for infusion is prepared by dissolving the content of one vial in up to 100 mL 0.9% sodium chloride for intravenous use.
40 mg dose: The reconstituted solution should be given as an intravenous infusion over a period of 10 to 30 minutes.
20 mg dose: Half of the reconstituted solution should be given as an intravenous infusion over a period of 10 to 30 minutes.
10 mg dose (Children 1-11 years): A quarter of the reconstituted solution should be given as an intravenous infusion over a period of 10 to 30 minutes.
1 mg/kg (Children 1-11 months*): Calculate the volume of the reconstituted solution for the required dose (1 mg/kg) and administer as an intravenous infusion over a period of 10 to 30 minutes.
0.5 mg/kg (Children 0-1 month*): Calculate the volume of the reconstituted solution for the required dose (0.5 mg/kg) and administer as an intravenous infusion over a period of 10 to 30 minutes.
*for definition of age for premature infants, see Pharmacology: Pharmacokinetics under Actions.
Continuous Infusion (40 mg vial): A solution for infusion is prepared by dissolving the content of two vials of esomeprazole 40 mg in up to 100 mL of 0.9% Sodium Chloride for intravenous use.
80 mg bolus dose: The reconstituted solution containing 80 mg esomeprazole should be given as a continuous intravenous infusion over 30 minutes.
8mg/hr dose: The reconstituted solution should be given as a continuous intravenous infusion over a period of 71.5 hours (calculated rate of infusion of 8 mg/hr).
Impaired renal function: Dose adjustment is not required in patients with impaired renal function. Due to limited experience in patients with severe renal insufficiency, such patients should be treated with caution (see Pharmacology: Pharmacokinetics under Actions).
Impaired hepatic function: GERD: Dose adjustment is not required in patients with mild to moderate liver impairment. For patients with severe liver impairment, a maximum daily dose of 20 mg Esomeprazole (NEXIUM) I.V. should not be exceeded.
Bleeding Ulcers: Dose adjustment is not required in patients with mild to moderate liver impairment. For patients with severe liver impairment, following an initial bolus dose of 80 mg Esomeprazole (NEXIUM) I.V., a continuous intravenous infusion dose of 4 mg/hr may be sufficient to maintain adequate acid control (see Pharmacology: Pharmacokinetics under Actions).
Elderly: Dose adjustment is not required in the elderly.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Sign Out
Sign Out